We know that all AOPA members are very interested in all health care reform efforts, as they have the potential to impact both the patients we serve, and how AOPA members plan and conduct their business. AOPA members who attended this year’s May Policy Forum had the opportunity to meet Senator Bill Cassidy (R-LA), and heard from him first hand his thoughts on how Congress might go about trying to attain universal health coverage in an alternative to the Affordable Care Act (ACA). While the Cassidy-Graham bill that emerged, and has dominated headlines in the past ten days, reflected some changes from the plan that Senator Cassidy had outlined at the Forum, it does reflect Senator Cassidy’s aspirations to move funding resources closer to the patient, while trying to come to grips with expansion of Medicaid coverage.
Because of the political impasse between Republicans and Democrats about the topic of “repeal and replace,” Republicans have sought to pursue legislation to address the ACA under the rules of “budget reconciliation,” which avoid the prospect of filibuster, and thereby avoid the need for 60 votes to bring debate to a close on a matter in the U.S. Senate. Because the federal government’s fiscal year ends, and the budget year concludes at midnight on Saturday evening, September 30, the opportunity to operate under these filibuster-proof rules expires at that time, and this in turn has generated a haste in trying to act on the Cassidy-Graham bill. Throughout this year, AOPA has viewed reform initiatives through the lens of impact on three patient-centric provisions: Cassidy-Graham would: (1) recognize the prospect of waivers available to states to modify the ACA’s essential health benefits (which could therefore impact the current “rehabilitative and habilitative essential benefit”); (2) patients with pre-existing conditions—including a substantial number of O&P patients—would be assured of being eligible for coverage, although state waivers might be invoked that could increase the cost of coverage for those with pre-existing conditions; and (3) Cassidy-Graham would shift Medicaid funds via block grants to the states in accordance with a formula, envisioning reduction of expansion of federal Medicaid funding over a period of years.
Right now, the outlook for Cassidy-Graham was mixed. With all 48 Senate Democrats aligned in opposition to the bill, and with at least three Republican Senators—Sens. Collins (R-ME), McCain (R-AZ) and Paul (R-KY)—stating that they intended to vote against the bill, the arithmetic looks adverse unless one of the Democrats or one of the three Republicans shifts position without any other Republicans gravitating to the opposition column. Clearly, this is an important deliberation in process, with the time pressures before September 30 limiting the extent of independent CBO analysis. We’ll keep AOPA members apprised of further significant developments on Cassidy-Graham and any other health reform initiatives.
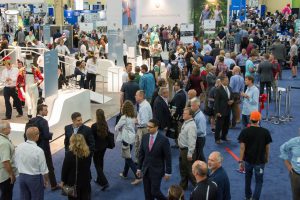
AOPA’s Centennial Celebration and World Congress in Las Vegas set a new record with over 2,500 attendees! Exhibitors and attendees came from 41 countries, making it a truly global event. AOPA is donating $5 of each registration to Hurricane Harvey relief, and is still accepting donations. Checks can be mailed to AOPA, 330 John Carlyle St, Ste 200, Alexandria, VA 22314.
The exhibit hall opened with a performance from the Las Vegas production La Reve- the Dream, with an impressive dancer doing backflips on a prosthetic leg.
The morning opening session presented Saeed Zahedi, PhD with the Lifetime Achievement awards and 4 notable inventors were honored for their contribution to O&P: Van Phillips (Flex-Foot); Marty Carlson, CPO(E), FAAOP (Tamarack Flexure Joint); M.E. “Bill” Miller, CO, (The Boston Brace System); and Kelly James, (C-Leg).
The educational line-up was described as our “best ever”, with presentations on Exosekeletons, Osseointegration, Gait Salvage, CMT, and all the latest clinical research. Business managers learned all about documentation, heard from the DME MACs, watched demos of the AOPA Co-OP, and more, while pedorthic and technical education covered all the latest topics.
As part of the Prosthetics 2020 research initiative, findings from the RAND Study “Economic Value of Advanced Transfemoral Prosthetics” were presented – that microprocessor knees (MPKs) provided economic benefits and quality of life improvement over non-MPKs. The study is now available on RAND’s website. Al Dobson, PhD presented the updated Dobson-DaVanzo cost-effectiveness study using the 2007-14 Medicare data, that found that O&P care is still cost-effective, similar to the 2007-10 data.
Attendees enjoyed the Walk through Time showcase in the Exhibit Hall, with artifacts and photos spanning O&P’s history. The Party with a Purpose fundraiser for AOPA’s government relations efforts brought in over $50,000, at an exclusive party at the 1923 Bourbon Bar Speakeasy. AOPA continued traditions of hosting a student Lunch and Learn, a Women in O&P gathering, and AOPA helped to facilitate Alumni meetups for 3 schools.
See all the photos on Flickr and search #AOPA2017 on Twitter.
La Reve performersExhibit HallFriday Morning Session on RAND StudyThe official magazine of the World CongressWalk through TimeWalk through TimeParty with a PurposeAOPA President Michael Oros
Washington, DC – In light of cost-cutting pressure from payers, in particular Medicare where total payments for prosthetics declined 15% during the 2010-14 period despite advances in technologies, and a 2015 attempt to tighten rules even more, there has been in urgent need to demonstrate the value of advanced prosthetics and related services. The RAND Corporation is a non-profit, non-partisan research institution respected for decades of key contributions to inform public policy debates, who undertook this needed comprehensive economic valuation for advanced prosthetics. The conclusion of RAND’s efforts serves as a marker that is answering not only specific questions about the costeffectiveness of technology utilization, but will also provide a P&O specific basis for a generation of researchers and health economists to build upon.
Due to recent advances in technologies, prosthetic knees and feet allow for more dynamic movements and improve user quality of life, but payers have recently started questioning their value for money. To answer this question, RAND undertook a study that simulated the differential clinical outcomes and cost of microprocessor-controlled knees (MPK) compared to non-microprocessor controlled knees (NMPK). We conducted a literature review of the clinical and economic impacts of prosthetic knees, convened technical expert panel meetings, compiled the input parameters required, and constructed and implemented a simulation model over a 10-year time period for unilateral transfemoral Medicare amputees with a Medicare Functional Classification Level of 3 and 4. RAND found that compared to NMPK, MPK is associated with sizeable improvement in physical function and reductions in incidences of falls and osteoarthritis. The effect on low-back pain, depression, obesity, diabetes, and cardiovascular disease could not be quantified due to the lack of data.
RAND’s study showed that 26% of patients who received more advanced prosthetic limbs with MPK will fall per year, contrasted to patients receiving non-MPK limbs, of whom 82% will fall per year. 10.4% of these are medical falls with a range of costs: 7% of these medical falls result in death (cost $27,338); 40% result in major injuries with inpatient and/or skilled nursing facility treatment (cost $23,363), and the remaining 53% have minor injuries (cost $1,091). There are 22 fall-related deaths per 10,000 patient years for the non MPK amputees, and 4 fall-related deaths per 10,000 patient years for the MPK amputees—18 lives saved by MPK usage. The simulation data show 66 injurious falls with the MPK, and 289 with the nonMPK. MPK amputees have a lower incidence of osteoarthritis due to lower vertical ground force (14% for MPK vs. 20% for non-MPK), although evidence is not robust. While MPK users have approximately $4,220 lower direct and indirect healthcare costs per year than non-MPK users, but the higher cost for the prosthesis itself exceeds that yearly savings. RAND’s simulation results show that over a 10-year time period, compared to NMPK, MPK is associated with an incremental cost of $10,604 per person and an increase of 0.91 quality adjusted life year per person, resulting in an incremental cost of $11,606 per quality adjusted life year gained. The results suggest that the incremental cost of MPK is in line with commonly accepted criteria for good value for money and with the incremental cost of other medical devices that are currently covered by U.S. payers.
In general terms, the RAND study followed rigorous, well-accepted methods for formal health care costeffectiveness analysis. This is a complex analytical endeavor, but the results are not too difficult to interpret. For a specific “event pathway” for treatment and outcomes, probabilities of results are calculated and summed up, as are the associated costs. A substantial measure that is used to convey the end result of the analysis is called an incremental cost effectiveness ratio. The incremental cost-effectiveness ratio equals the difference (increment) in cost divided by the difference (increment) in effectiveness or outcome between alternative treatments. The outcome is just as important as cost. If you have better outcomes, this improves the cost effectiveness ratio just as much as decreasing cost would.
A scientific study seeks to answer carefully specified questions, and we must be careful not to generalize beyond the data we have. For example, in the current study RAND could only draw firm conclusions where there is sufficient published peer reviewed data already available. The continued collection and publication of high-quality data about our patient populations, alternative treatments and outcomes is essential.
MPK microprocessor controlled knee; TKA: total knee arthroplasty; ICD: implantable cardioverter defibrillator. The reference ICER ratios are based on lifetime benefits whereas the ICER of MPK is for a 10-year time period. Institute for Clinical and Economic Review’s criteria are used to judge value.
Questions? Please contact Lauren Anderson, AOPA’s Manager of Communications, Policy, and Strategic Initiatives at 571/431-0843 or landerson@aopanet.org.
WASHINGTON, D.C. – The 99th Annual AOPA National Assembly is coming to the Hynes Convention Center in Boston, MA. The Annual Assembly is the highlight of the year for the more than 2,200 orthotic, prosthetic and pedorthic professionals expected in attendance – because of its expansive educational opportunities, massive exhibit hall, and engaging events.
AOPA is proud to unveil Expo Day in the 100,000 square foot exhibit hall, where there will be special events, patient demonstrations and lots of door prizes. Special guests at Expo Day include Jeff Bauman, who became an amputee during the 2013 Boston Marathon Bombing and played a vital role in identifying the bombers. He will be signing copies of his memoir, Stronger to benefit the Wiggle your Toes Foundation. Professional ballroom dancer and bombing survivor Adrianne Haslet-Davis will perform for the crowd and teach interested participants the Waltz or the Rumba.
The much anticipated Boston Strong Grand Rounds will begin with Adrianne and Heather Abbott sharing their stories of recovery since the bombing. Then a multidisciplinary panel will review three actual case studies of amputee survivors with the medical teams who cared for them. The panel will be moderated by Dr. David Crandell of Spaulding Rehabilitation Hospital, who was involved in the care of 25 of the most severely injured survivors of the bombing, including 15 amputees. The panel includes surgeons, prosthetists and physical therapists from Spaulding, Boston Medical Center, Atrius Health, Brigham & Women’s, Medical Center O&P, and Hanger Clinic.
Another anticipated program is the session on Osseointegration, a relatively new procedure where a titanium rod is implanted in the bone of the residual limb to attach a prosthetic limb, instead of a traditional socket. The procedure is being used by only a few surgeons worldwide, and several will be on the panel for this discussion.
The full schedule for the Assembly is online at www.AOPAnet.org.
Event times and locations:
Expo Day- Saturday, September 10, 10:00 AM-2:00 PM
Jeff Bauman book signing with proceeds benefiting Wiggle Your Toes. Location: Auditorium, Aisle 500 Time: 10:00 AM-2:00 PM
Adrianne Haslet-Davis dance performance Location: Booth 1629, Hall D Time: 10:15 AM
Adrianne Haslet-Davis Dance Instruction Location: Booth 1629, Hall D Time: 10:30 AM
Education Highlights:
Sept. 9, 2:00 pm: About Osseointegrated, Percutaneous Implants for Rehabilitation following Limb Amputation
Sept. 10, 2:00 pm: Boston Strong Grand Rounds
Sept. 9, 7:30 am: Keynote #1 with Sen. Bob Kerrey
Sept. 9, 11:30 am: Keynote #2 with David Gergen, CNN Senior Political Analyst
On July 13, 2017, the DME MACs published a joint publication that addressed the proper use of HCPCS code A5513, which is used to described molded to patient model diabetic shoe inserts.
The joint publication indicated that in order to meet the requirements of the HCPCS code descriptor, diabetic inserts billed using A5513 must be molded over an actual model of the patient’s foot. The publication further clarified that the use of generic, electronic or “virtual” models where custom fabrication occurs without creation of a physical model of the patient’s foot does not meet the code descriptor, and diabetic inserts fabricated this way cannot be billed as A5513.
On August 10, 2017, the Pricing, Data Analysis, and Coding Contractor (PDAC) announced that based on the previously published coding clarification, it would initiate a Coding Redetermination Project for diabetic inserts described by A5513. As part of this project, all previous A5513 PDAC coding verifications will be end dated effective May 31, 2018. Manufacturers and central fabrication facilities who wish to have their products PDAC verified for A5513 will need to submit a new application to the PDAC. This applies to both new products as well as existing products that were previously verified by the PDAC. The PDAC has indicated that applications should be submitted well in advance of the May 31, 2018 end date in order to allow adequate time for the PDAC to complete its review.
The PDAC notice stated that products that are currently PDAC verified for A5513 may continue to be billed using A5513 until the May 31, 2018 end date. Medicare claims for diabetic inserts described by A5513 with a date of service on or after June 1, 2018 will require a new PDAC coding verification using the requirements outlined in the July 13, 2017 coding clarification.
As a reminder, AOPA members who are fabricating diabetic inserts described by A5513 for use by their own patients are not required to obtain PDAC verification but must meet the requirements of the code descriptor which includes the creation of a positive model of the patient’s foot. View the complete PDAC announcement.
This afternoon, the full House of Representatives acted by consent on suspension to adopt H.R. 3178, a bill to cut red tape and make some non-controversial changes to the Medicare program. Included in this bill was a single provision on O&P– the long-awaited provision to recognize the orthotist-prosthetist’s notes as part of the medical record in Medicare Medical Necessity Determinations. Here is the specific text as enacted by the House:
1 SEC. 103. ORTHOTIST’S AND PROSTHETIST’S CLINICAL NOTES AS PART OF THE PATIENT’S MEDICAL RECORD.
Section 1834(h) of the Social Security Act (42 U.S.C. 1395m(h)) is amended by adding at the end the following new paragraph:
”(5) DOCUMENTATION CREATED BY ORTHOTISTS AND PROSTHETISTS.- For purposes of determining the reasonableness and medical necessity of orthotics and prosthetics, documentation created by an orthotist or prosthetist shall be considered part of the individual’s medical record to support documentation created by eligible professionals described in section 1848(k)(3)(B).”
AOPA wants to recognize and thank Reps. Mike Bishop (R-MI and a Ways & Means member), Glenn Thompson (R-PA) who advanced the similar provision as part of the broader Medicare O&P Improvement Act, H.R. 2599, and Mike Thompson (D-CA and a Ways & Means Committee Member), and both House Ways & Means Committee Chairman Kevin Brady (R-TX) and Richard Neal (D-MA and the Ranking Minority Member of the Ways & Means Committee), for their strong support which resulted in this important action. Now it is on to the Senate, where S. 1191, the Grassley-Warner bill, supported by Senators Cassidy (R-LA) and Duckworth (D-IL) will hopefully move forward similarly to favorable action.
In conjunction with our continuing efforts to advance the provisions of H.R. 2599/ S.1191, the Medicare Orthotics & Prosthetics Improvement Act, we are pleased to advise you that the provision which would assure that the prosthetist/orthotist patient notes are included as part of the official Medicare medical record for purposes of medical necessity determinations has been picked up in a larger bill, H.R. 3178, which has been approved and recommended by vote of the House Ways and Means Committee on Thursday, July 13, to the entire House for favorable action.
Clearly, if the expected approval by the entire House ensues, a similar action by the entire Senate would be required before the measure would go to the President for signature. There has been strong interest in the Senate Finance Committee in enacting S.1191 in its entirety, hopefully later this year. Thursday’s action by the Ways and Means Committee, linked below, is very encouraging, and we both appreciate the strong support AOPA members and their patients have voiced for H.R. 2599/ S.1191; AOPA will keep you informed of additional steps toward enactment.
GROUPS: AMPUTEES HAVE MUCH TO LOSE IF HEALTH CARE REFORM UNDERCUTS KEY ASPECTS OF SAFETY NET
WASHINGTON, D.C. – Many of the two million Americans who are amputees – including military veterans, accident victims, and older Americans – could lose care and the mobility and liberty that comes with that care if federal health care reform is not crafted to avoid three key “pitfalls,” according to the American Orthotic & Prosthetic Association (AOPA) and the Amputee Coalition.
As outlined by the groups in a Tuesday news conference, the “big three” priority issues for amputees are as follows: (1) no cuts to Medicaid that would turn back the clock on the limb-loss/mobility impaired community in terms of access to needed treatment and state-of-the-art devices; (2) no waivers as to rehabilitative and habilitative services (an essential health benefit) that could be used to deny access to care and treatment for amputees; and (3) no changes to authorize higher premiums with respect to amputation as a pre-existing condition that could interfere with coverage access. (See details below.)
AOPA President Michael Oros said: “For amputees, loss of affordable health insurance not only means a loss of care, it also means a loss of independence and liberty in the form of the mobility that the care makes possible. AOPA and the Amputee Coalition are also concerned about the tendency of the insurance industry to use discussion of the potential for any cuts as the basis denial of service, even when bills or regulations are not enacted. We are talking about two million Americans here, many of whom are gainfully employed, paying mortgages and raising families, and actively involved in their communities.”
Dr. Jeff Cain, head of advocacy program of the Amputee Coalition, a Denver physician, and former president, American Academy of Family Physicians, said: “Arms and legs are not a luxury … I have three concerns about the current health care reform that could severely limit people with amputations: #1) If fewer people have insurance, fewer people can afford health care, and that means fewer amputees will be able to afford a leg to stand on … second, not mandating essential health benefits, including habilitative and rehabilitative services, would mean that the cost to insure those people would rise dramatically. If you can’t afford an insurance policy, you can’t afford a leg to stand on … and third, we cannot afford to go back to the pre-ACA world of pre-existing conditions, which prevented amputees across the country from being able to afford a leg to stand on.”
More details about the three areas of concern for AOPA and the Amputee Coalition are detailed here:
Medicare cuts. Orthotics and prosthetics provided through Medicaid to millions of individuals are at risk within the current framework of healthcare legislation reform. In 2013, around the time the Medicaid expansion was in full effect, the recorded number of amputations (upper and lower extremity) was 154,000 and 14% of those where paid by Medicaid as compared to 18% by private payers. Since the majority of amputations are between the ages of 45-64, the time before someone becomes eligible for Medicare, and the fact that not all private payers cover prosthetics, the loss of Medicaid expansion could be detrimental to patients facing limb loss and already suffering from limb loss.
Essential health benefits. Removing of certain essential health benefits from insurer plans may cause individuals to face the possibility of not having coverage for orthotics and prosthetics (bracing and artificial limbs), or be faced with unrealistic annual limits or artificial lifetime caps. Orthotics and prosthetics are considered an essential health benefit under the rehabilitative and habilitative services and devices category; in part because it was included in 70-75 percent of private payer plans. If essential health benefits are removed we could return to 25-30% or more of private employer plans not covering orthotics and prosthetics, and possibly even an increase in the number of non-employer based plans not including O&P coverage.
Pre-existing conditions. Amputations which are traumatic or caused by an accident, may not always be considered a pre-existing condition, however if the amputation and all follow-up care is required as a result of a disease (non-traumatic); then it could be considered as a pre-existing condition. For example, diabetes may be curable but can also be a long-term illness and lead to an amputation; and cause insurance companies to declare the amputation as a pre-existing condition. A large number of individuals have been affected by the burdens caused by diabetes, in 2010 29.1 million individuals were diagnosed with diabetes and in 2010 60% of non-traumatic lower-limb amputations among adults were attributed to people with diabetes. There are also several conditions (e.g. cerebral palsy or multiple sclerosis) currently listed as pre-existing, and life lasting, which may result in some type of limb impairment and require the use of an orthosis.
GROUPS: AMPUTEES HAVE MUCH TO LOSE IF HEALTH CARE REFORM UNDERCUTS KEY ASPECTS OF SAFETY NET
WASHINGTON, D.C.///June 29, 2017///Many of the two million Americans who are amputees – including military veterans, accident victims, and older Americans – could lose care and the mobility and liberty that comes with that care if federal health care reform is not crafted to avoid three key “pitfalls,” according to the American Orthotic & Prosthetic Association (AOPA) and the Amputee Coalition.
As outlined by the groups in a Tuesday news conference, the “big three” priority issues for amputees are as follows: (1) no cuts to Medicaid that would turn back the clock on the limb-loss/mobility impaired community in terms of access to needed treatment and state-of-the-art devices; (2) no waivers as to rehabilitative and habilitative services (an essential health benefit) that could be used to deny access to care and treatment for amputees; and (3) no changes to authorize higher premiums with respect to amputation as a pre-existing condition that could interfere with coverage access. (See details below.)
AOPA President Michael Oros said: “For amputees, loss of affordable health insurance not only means a loss of care, it also means a loss of independence and liberty in the form of the mobility that the care makes possible. AOPA and the Amputee Coalition are also concerned about the tendency of the insurance industry to use discussion of the potential for any cuts as the basis denial of service, even when bills or regulations are not enacted. We are talking about two million Americans here, many of whom are gainfully employed, paying mortgages and raising families, and actively involved in their communities.”
Dr. Jeff Cain, head of advocacy program of the Amputee Coalition, a Denver physician, and former president, American Academy of Family Physicians, said: “Arms and legs are not a luxury … I have three concerns about the current health care reform that could severely limit people with amputations: #1) If fewer people have insurance, fewer people can afford health care, and that means fewer amputees will be able to afford a leg to stand on … second, not mandating essential health benefits, including habilitative and rehabilitative services, would mean that the cost to insure those people would rise dramatically. If you can’t afford an insurance policy, you can’t afford a leg to stand on … and third, we cannot afford to go back to the pre-ACA world of pre-existing conditions, which prevented amputees across the country from being able to afford a leg to stand on.”
More details about the three areas of concern for AOPA and the Amputee Coalition are detailed here:
Medicare cuts. Orthotics and prosthetics provided through Medicaid to millions of individuals are at risk within the current framework of healthcare legislation reform. In 2013, around the time the Medicaid expansion was in full effect, the recorded number of amputations (upper and lower extremity) was 154,000 and 14% of those where paid by Medicaid as compared to 18% by private payers. Since the majority of amputations are between the ages of 45-64, the time before someone becomes eligible for Medicare, and the fact that not all private payers cover prosthetics, the loss of Medicaid expansion could be detrimental to patients facing limb loss and already suffering from limb loss.
Essential health benefits. Removing of certain essential health benefits from insurer plans may cause individuals to face the possibility of not having coverage for orthotics and prosthetics (bracing and artificial limbs), or be faced with unrealistic annual limits or artificial lifetime caps. Orthotics and prosthetics are considered an essential health benefit under the rehabilitative and habilitative services and devices category; in part because it was included in 70-75 percent of private payer plans. If essential health benefits are removed we could return to 25-30% or more of private employer plans not covering orthotics and prosthetics, and possibly even an increase in the number of non-employer based plans not including O&P coverage.
Pre-existing conditions. Amputations which are traumatic or caused by an accident, may not always be considered a pre-existing condition, however if the amputation and all follow-up care is required as a result of a disease (non-traumatic); then it could be considered as a pre-existing condition. For example, diabetes may be curable but can also be a long-term illness and lead to an amputation; and cause insurance companies to declare the amputation as a pre-existing condition. A large number of individuals have been affected by the burdens caused by diabetes, in 2010 29.1 million individuals were diagnosed with diabetes and in 2010 60% of non-traumatic lower-limb amputations among adults were attributed to people with diabetes. There are also several conditions (e.g. cerebral palsy or multiple sclerosis) currently listed as pre-existing, and life lasting, which may result in some type of limb impairment and require the use of an orthosis.
ABOUT THE GROUPS
The American Orthotic & Prosthetic Association (www.aopanet.org) is a national trade association committed to providing high quality, unprecedented business services and products to O&P professionals. Since its founding in 1917, AOPA has worked diligently to establish ourselves as the voice for O&P businesses. Through government relations efforts, AOPA works to raise awareness of the profession and impact policies that affect the future of the O&P industry. AOPA membership consists of more than 2,000 O&P patient care facilities and suppliers that manufacture, distribute, design, fabricate, fit, and supervise the use of orthoses (orthopedic braces) and prostheses (artificial limbs).
Amputee Coalition (http://www.amputee-coalition.org/) is a nationwide voluntary health organization dedicated to ensuring no amputee feels alone and that amputees and their families have the resources they need to recover, readjust and live life fully with limb loss/difference. Headquartered in the Greater Washington DC Area in Manassas, Virginia, we have more than 300 support groups in our network, more than 1,000 certified peer visitors across the country, and more than 65,000 friends in our database.
MEDIA CONTACT: Patrick Mitchell, (703) 276-3266 and pmitchell@hastingsgroup.com.
Ann McSweeney, a Chicago area mother of twins who both wear orthoses on lower extremities and one spinal as well.
https://video214.com/play/0cnidvYSpld50IWoxXJiiw/s/dark
Kelly Miller, an amputee from the Baltimore, MD area
https://video214.com/play/TYQtlkpF3jBcyRDAc2cUgw/s/dark
Adrianne Haslet, world class ballroom dancer, Boston Marathon bombing survivor, and amputee rights advocate
Subscribe to the July-December half-year series and get 3 free webinars. This includes 2 bonus webinars added as part of Healthcare Compliance & Ethics Week, that are free to all AOPA members with no purchase required.
Stay on top of all relevant reimbursement issues and earn 1.5 CE credits each month. One registration is all it takes to provide the most reliable business information for your entire staff.
Just $495 members/$995 non-members for all 8 webinars! Individual webinars are $99 AOPA members/$199 non-members.
Register now.
July 12
Know Your Resources: Where to Look to Find the Answers
August 9
What the Medicare Audit Data Tells Us & How to Avoid Common Errors
September 13
ABC Inspections & Accreditation
October 11
AFO/KAFO Policy
November 8
Gift Giving: Show Your Thanks & Remain Compliant
November 9*
“Three Amigos” of a Compliance Program- Compliance Officer, Legal, and Human Resources-Can Work Together to Support and Advance an Effective Compliance Program
November 10*
Teaching Professionalism and Ethics during Residency
December 13
New Codes & Other Updates for 2018
*These webinars are free to all AOPA members as part of Healthcare Compliance & Ethics Week Webinar; and $50 for non-members.









 Subscribe to the July-December half-year series and get 3 free webinars. This includes 2 bonus webinars added as part of Healthcare Compliance & Ethics Week, that are free to all AOPA members with no purchase required.
Subscribe to the July-December half-year series and get 3 free webinars. This includes 2 bonus webinars added as part of Healthcare Compliance & Ethics Week, that are free to all AOPA members with no purchase required.